This blog series is part of an ongoing study by Data2X and Open Data Watch to track the gender impacts of COVID-19. We recently published a report on the availability of sex-disaggregated data for tracking the primary and secondary impacts of the pandemic. Learn more in our summary blog post and full technical report, Tracking the Gender Impact of COVID-19: An Indicator Framework. This blog post originally appeared on Open Data Watch’s website.
In this blog, we summarize the existing data on sex-disaggregated COVID-19 cases and deaths from Global Health 50/50 and ask how complete our picture is when compared to all reported cases and deaths. In addition, we examine the shares of COVID-19 cases and deaths that are sex-disaggregated by income group.
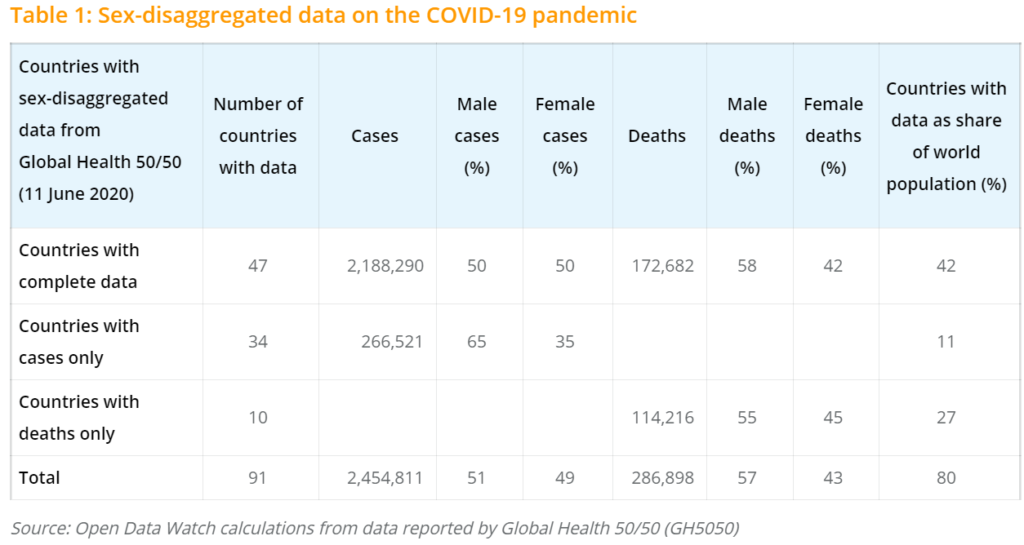
Table 1 summarizes the sex-disaggregated data available as of 11 June 2020 from GH5050. Since last week’s post, 8 countries were added to the database with information on sex-disaggregation: Albania, Costa Rica, Central Africa Republic, Cuba, Ethiopia, Kyrgyzstan, Lebanon, and Paraguay. Two further countries, Haiti and North Macedonia, added sex-disaggregated information on deaths to their existing information on cases.
In total, there were 47 countries reporting sex-disaggregated data for COVID-19 cases and deaths. (These include three nations of the United Kingdom – England, Scotland, and Northern Ireland – that are reported separately. Wales reports cases only.) They represented 42 percent of the world’s population (2019 data). 10 countries report sex-disaggregated data for deaths only. 34 more countries report sex-disaggregated data on cases but lack data on deaths. In total, 4 out of 5 people now live in a country with at least some sex-disaggregated data on COVID-19. For countries reporting all sex-disaggregated data, women make up 50 percent of cases but only 42 percent of deaths.
Although stories about reported cases and deaths caused by the COVID-19 virus have mainly covered high-income countries, information about the pandemic in low- and lower-middle-income countries is slowly emerging and will be crucial to monitoring the impacts of the pandemic on development efforts and the 2030 Agenda. As of 11 June 2020, 5 low-income countries published sex-disaggregated data (Central African Republic, Ethiopia, Somalia, and Nepal on cases only, Haiti on both). Sex-disaggregated data is available for 15 lower-middle-income countries.[1] See Table 3 below for a more in-depth discussion on the reporting of deaths and cases by income group.
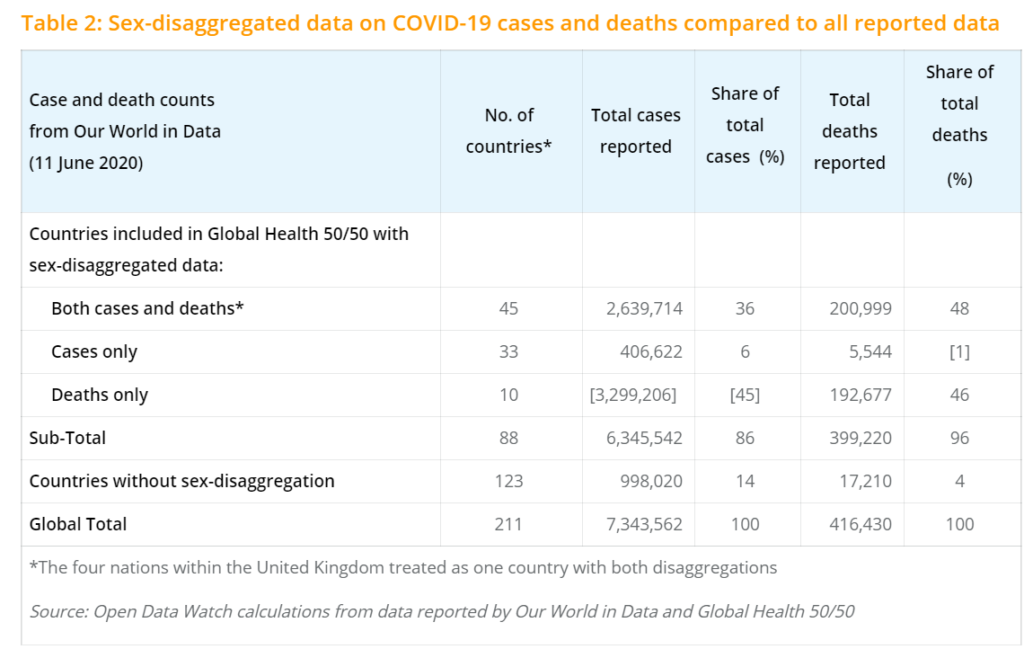
Table 2 summarizes the number of cases and deaths compiled by the European CDC and reported by Our World in Data (OWID) for the countries with sex-disaggregated data and for the remaining 123 countries that currently lack any sex-disaggregated data. (Figures in square brackets are for countries that report either cases or deaths but not both in GH5050. Data for the four nations of the United Kingdom are included in Table 2 as a single country reporting sex-disaggregated cases and deaths.)
The countries included in the current GH5050 database account for 86 percent of global cases and 96 percent of deaths. However, when accounting for countries publishing only case or death information, the shares drop to 41 percent and 95 percent, respectively.[2] This adjustment reveals that deaths are nearly all sex-disaggregated, while only 2 in 5 cases are actually sex-disaggregated, a ratio that would double to 4 in 5 if Brazil and the United States reported their cases by sex.
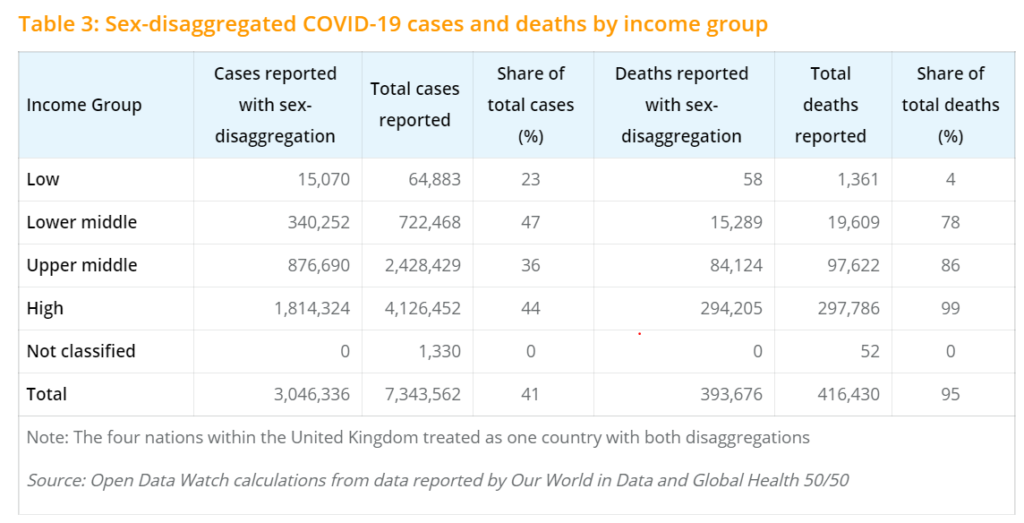
To arrive at a more nuanced understanding of the way in which countries report on COVID-19 cases and deaths, we analyzed the global shares according to World Bank FY2020 income groups in Table 3. Though only 5 low-income countries report on deaths and cases in GH5050, we can say that their capacity to report on these indicators by sex remains low. On the other hand, lower-middle-income countries report more of their cases by sex as a share than any other income group. This is again driven by the absence of sex-disaggregation of cases by two countries with some of the largest caseloads in the world. If Brazil’s nearly 780,000 cases were sex-disaggregated, the share of cases reported by sex for upper-middle-income countries would rise to 68 percent, and if the United States’ 2 million cases were sex-disaggregated, the share of cases for high-income countries would more than double to 92 percent. Reporting on deaths by sex, meanwhile, reveals the most straightforward correlation between statistical capacity and income. High-income countries report practically all their deaths by sex and this share declines with each step down the income group ladder.
Next week, the blog will update the global tables above and examine the sex-disaggregated status of COVID-19 cases and deaths by region.